

Editor's Note: We have updated some of the analysis from this 2018 report in a more research brief released on September 17, 2021. Please read it at: Opioid-Related Deaths in Massachusetts Remain Elevated Four Years after Peak.
By Anise Vance and Luc Schuster
The opioid crisis has received a good deal of public attention, and appropriately so. But its scale may be even worse than you realize. Opioid-related deaths have increased dramatically over the past few years, and the opioid-related death rate in Massachusetts is now more than twice the national rate. To support the design of smart, tailored public responses, this research brief is organized into two short sections: 1) we put the size of the opioid crisis into context; and 2) we analyze the best available data to understand why the crisis has been increasing faster in Massachusetts than in most other states. Key findings include (click to jump to section):
- Fentanyl has become more common in Massachusetts, especially illicit fentanyl.
- There is likely a regional effect at play, with most New England states all having high opioid-related death rates.
- Key Northeast drug trafficking routes run through Massachusetts.
- Economic hardship is related to opioid use, but it doesn’t explain the recent increase.
- Doctor-prescribed opioids play a key role, but they don’t explain why Massachusetts has an opioid-related death rate twice the national average.
- Heroin also plays a key role, but not to a degree that is significantly different from other states.
The Opioid Crisis in Context
Nationwide, over 42,000 people died from opioid-related causes in 2016, five times the number of opioid-related deaths in 2000.
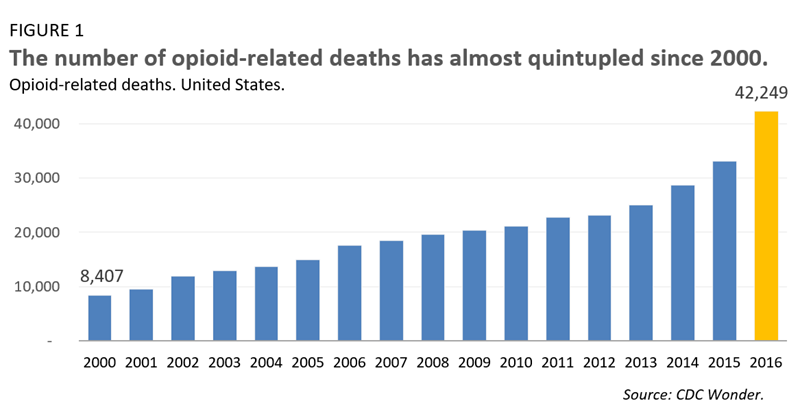
Comparing the current opioid crisis to other major causes of unnatural deaths provides some useful context on its scale:
- Roughly the same number of people died of opioid-related causes in 2016 as died from HIV/AIDS in 1995, the height of the HIV/AIDS epidemic.
- More people died from opioid-related causes than from motor vehicle accidents in 2016 (40,327).
- Driven by the opioid epidemic, more Americans died from drug overdoses in 2016 than the number of Americans who died fighting in the entire Vietnam War.
The opioid crisis is one key reason that life expectancy has fallen for the second year in a row. That last time life expectancy fell in back-to-back years was in 1962 and 1963, when influenza caused an unusual amount of deaths.
In Massachusetts, the opioid crisis is particularly acute. The opioid-related death rate in the Commonwealth is more than twice the national average. Up until 2012, Massachusetts hovered just above the national average, but a recent spike has led the gap to widen considerably.
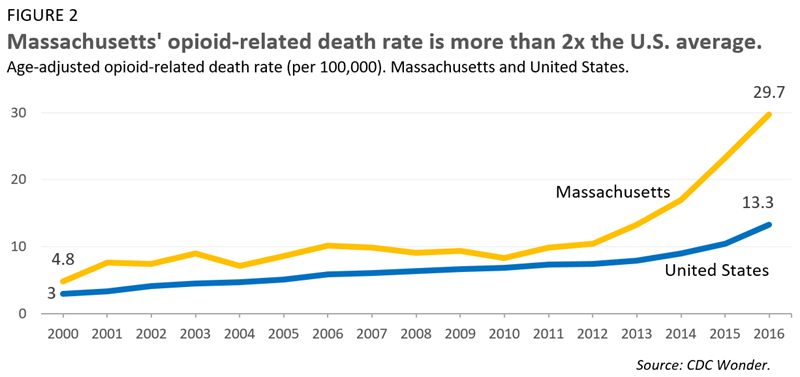
After steady increases from 2000 to 2012, our state’s opioid-related death rate has almost tripled in just four years—from 691 in 2012 to 1,990 in 2016. However, with such an active and fast-moving crisis, things can change in a hurry. The past year brought some limited good news: in 2017, opioid-related deaths dropped 6 percent in comparison to 2016. Early estimates of 2018 data suggest we may have seen some additional modest progress.
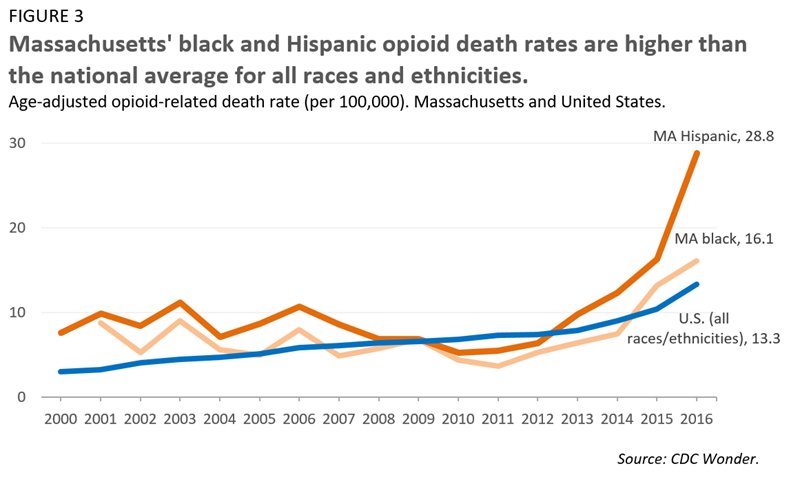
The opioid crisis has often been framed mostly, or even exclusively, as a problem afflicting the white population. During the early 2000s, however, the opioid-related death rate among the black and Hispanic populations in Massachusetts was about as high as that of the white population. The death rate among whites did spike in the late 2000s, but we are now seeing similar spikes for Massachusetts’ communities of color. In fact, Massachusetts’ black and Hispanic populations already have opioid-related death rates well above the national average for all races. And while opioid-related death rates have generally declined over the last year, the opioid-related death rate for the black population actually rose.
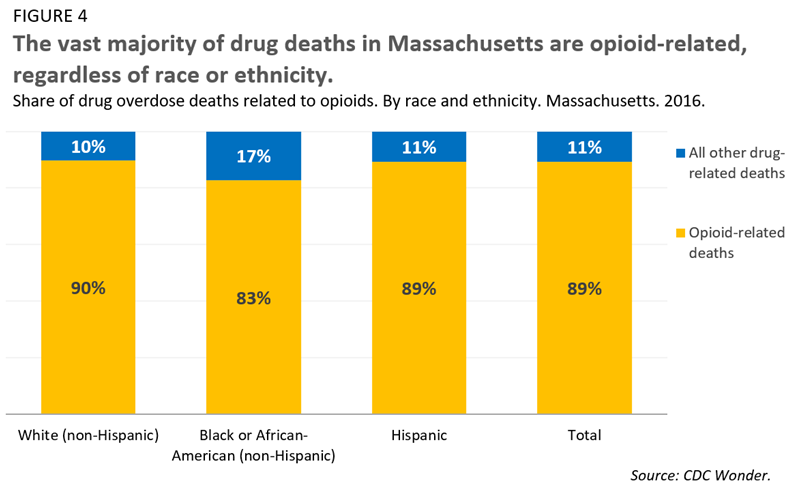
Currently, more than 80 percent of drug-related deaths in the white, black, and Hispanic communities are opioid related. The crisis—as the data clearly demonstrates—is not an exclusively white problem. It is a challenge that must be addressed by and for all of Massachusetts’ communities.
Why has the problem been worsening in Massachusetts?
Next, let’s dive into the data on what might explain why the opioid crisis has accelerated so rapidly in Massachusetts. We start by describing some likely causes and end by describing why a few common theories do not appear to be supported by the data.
Fentanyl has become more common in Massachusetts, especially illicit fentanyl.
First, what is fentanyl? Fentanyl is an opioid that can be prescribed, but is often produced and distributed illicitly. It has become popular among street drug dealers, in large part, because it is much more lucrative than heroin. Unlike prescription opioids or heroin, fentanyl is not usually taken on its own but, rather, is used to make other drugs more potent. Since it’s not used as a standalone drug, users are often unaware they are taking it, a lack of knowledge that is particularly problematic considering that fentanyl can be 50 times more potent than heroin and 100 times stronger than morphine. More troubling still, other synthetic drugs similar to and sometimes stronger than fentanyl, like carfentanil, continue to emerge.
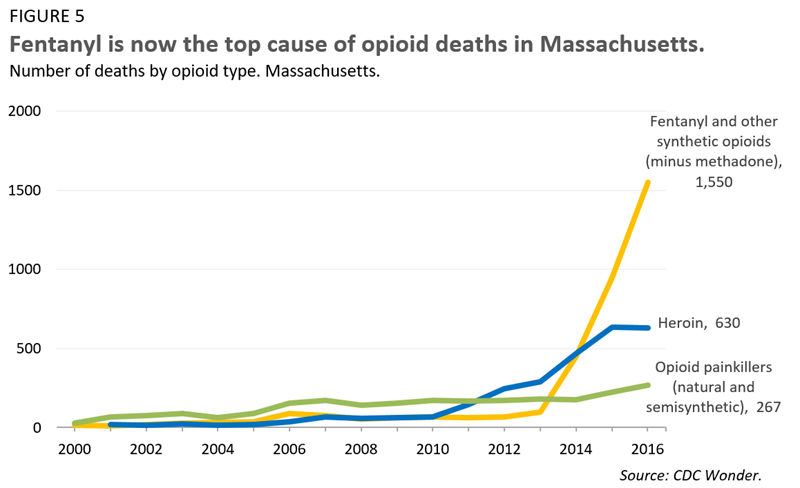
Nationally, fentanyl has become increasingly prevalent, overtaking heroin and opioid painkillers as the most common drug in opioid-related overdose deaths.1 In 2016, 19,413 people died from opioid-related deaths involving fentanyl or other non-methadone synthetics, more than six times the corresponding number from 2013.
While fentanyl use has increased nationally, the spike has been even more pronounced in Massachusetts. In 2016, there were 1,550 fentanyl-related deaths in Massachusetts, up from only 98 in 2013.2 This especially pronounced spike in fentanyl usage in Massachusetts explains in large part why our opioid-related death rate now far outpaces the national rate.
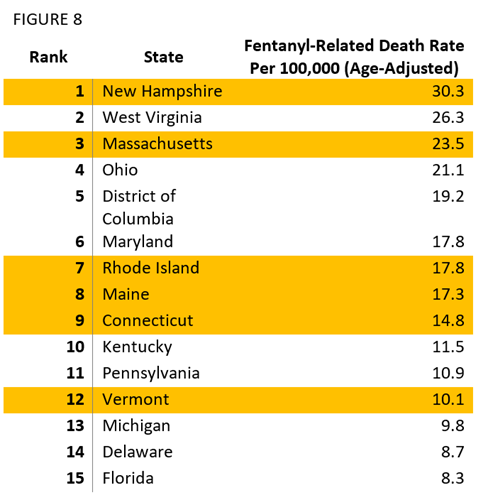
Fentanyl’s presence in Massachusetts is brought into even greater relief when compared to other states. Massachusetts has the third highest fentanyl-related death rate in the country, second only to New Hampshire and West Virginia.

Other evidence not specific to opioid-related deaths also suggests that Massachusetts has a particularly severe challenge with fentanyl. In 2017, Massachusetts had the second-highest number of fentanyl-related law enforcement reports, behind only Ohio. According to the National Drug Threat survey, distributed by the Drug Enforcement Agency to field offices, a larger share of New England field officers feel that fentanyl a the greater threat to their region than in any other part of the country.
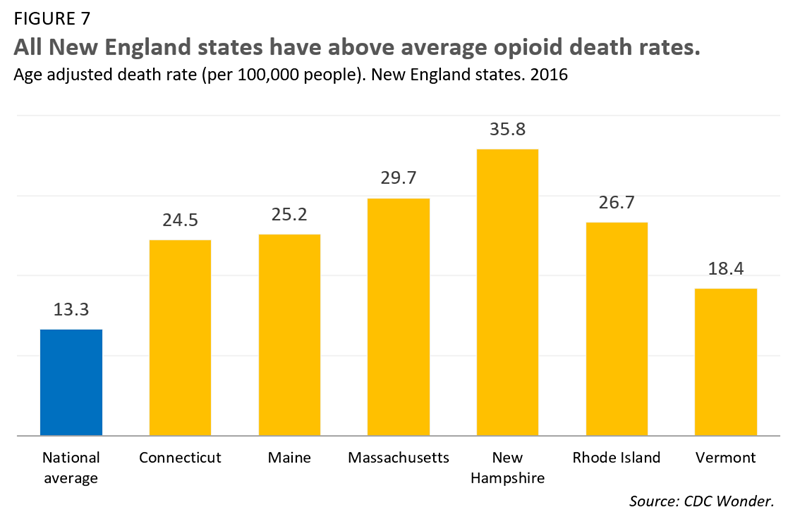
But what explains why fentanyl (and other illicit opioids) is so much more prevalent in Massachusetts? There appears to be a regional effect at play. Opioid-related deaths are not just high in Massachusetts, they are relatively high throughout New England. All six New England states have opioid-related death rates above the national average, and five of the six have death rates roughly double the national average.
Fentanyl is also relatively common in New England. Five of six New England states are in the top 10 in fentanyl-related death rates, and all six are in the top 15.
All six states are also in the top 15 for their share of opioid-related deaths connected to fentanyl, suggesting that New England in general is disproportionately affected by fentanyl.
Key Northeast drug trafficking routes run through Massachusetts.
Fentanyl, and other synthetic opioids, are often produced illicitly and trafficked across the country. Well prior to the current opioid epidemic, there were established and frequently used drug routes in New England, with Massachusetts as one of the region’s primary hubs. This, unfortunately, made Massachusetts more vulnerable than other places to the current stage of the opioid epidemic, when the trafficking of illicit fentanyl is of great consequence.
Transnational criminal organizations (TCOs) in the Northeast are particularly active and well-established. Critically, many of them often have the necessary infrastructure to both move drugs between states and sell directly to users. Over the past few years, there has also been increasing competition from TCOs expanding into the Northeast.
Today, Lawrence and Lowell are centers of the opioid trade for the region, and fentanyl has featured prominently in that trade. In 2016, the New England Drug Enforcement Agency seized a large heroin mill in Lawrence, where heroin and fentanyl were being mixed. In the same year, one of the largest cocaine and fentanyl mixtures was seized in Methuen.
Economic hardship is related to opioid use, but it doesn’t explain the recent increase.
Harsh economic conditions have certainly contributed to the opioid epidemic. As researchers have noted, deaths of despair are connected to a rise in various high risk behaviors, including drug use.
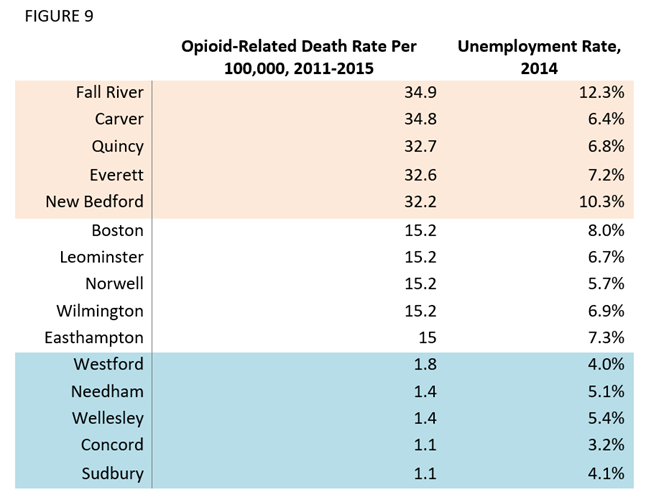
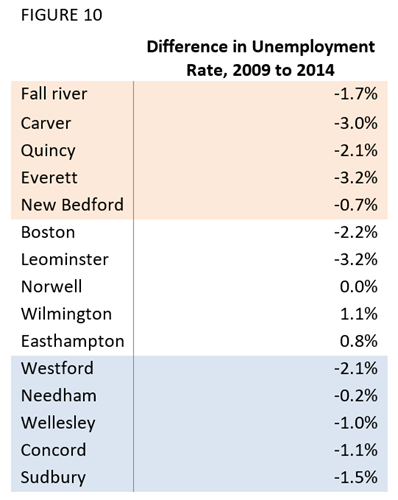
Among Massachusetts cities and towns with working populations over 5,000, the five places with the highest opioid-related death rates had unemployment rates significantly higher than the five places with the lowest opioid-related death rates. 3 4
Boston and the four towns immediately following it in opioid-related death rates had rates about midway between the highest and lowest ends of the spectrum. In 2014, they also had unemployment rates midway between places with the highest and lowest opioid-related death rates.
But, curiously, the opioid epidemic worsened over the past five or six years, years in which the economy was largely recovering from the Great Recession. If the opioid epidemic was being driven by poor economic conditions, we would have expected to see the opposite trend. Nuanced analysis of national data indicates that economic decline is associated with drug-related death—but the relationship is not strong enough to explain the scale of the opioid epidemic, especially the increase in recent years.
Massachusetts data seems to confirm this relationship. From 2009 to 2014, the unemployment rate dropped across places with the highest, middle-of-the-pack, and lowest opioid related death rates in the state. The unemployment rate has actually dropped most in places with the highest opioid-related death rates. As with the national story, this trend is opposite what we would expect if economic circumstance was the primary cause of the opioid epidemic.
The United States is unique in its broad use of opioids to address pain. In the 1990s, medical institutions and associations advocated for the use of prescription opioids as a safe antidote to pain, particularly after the introduction of OxyContin. Those same prescription opioids became a key factor, if not the key factor, in the initial rise of the opioid epidemic. Nationally, deaths from prescription opioids have quadrupled since 1999. In general, the more opioid prescriptions providers write, the larger the population of people who will develop addictions and the more pills will make their way to the illicit market.
But does a long-term uptick in prescriptions explain the difference between Massachusetts’ opioid-related overdose death rate and the national average? Probably not.
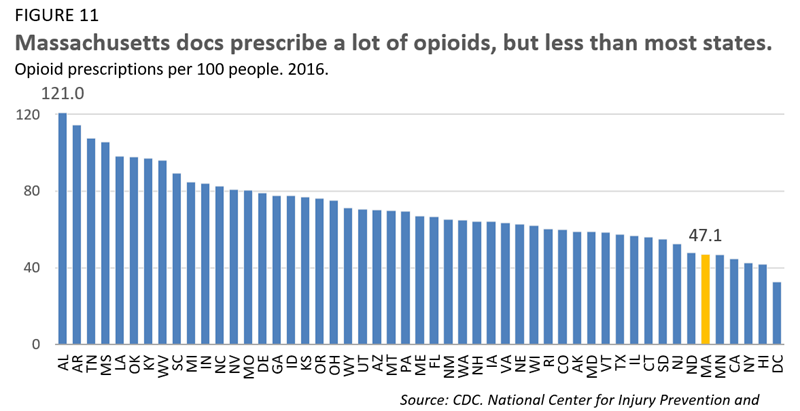
In 2016, there were 47.1 opioid prescriptions per 100 people in Massachusetts. That was the 5th lowest figure among states. In 2012, Massachusetts ranked 9th lowest and in 2008 it ranked 16th lowest. If opioid prescriptions were the driving factor in Massachusetts’ opioid-related death rate, we would not have expected to see a sharp rise in the death rate while the prescription rate was low (relative to other states)—and dropping lower still.
It is important to note that not all opioid prescriptions are created equal. Patients who take long-acting (or “extended release”) opioids are two to five times more likely to wind up addicted to opioids than are those who take other types of opioids.
So are more long-acting opioids prescribed in Massachusetts than in other states? The best data says, no. Massachusetts had the 7th lowest long-acting opioid prescription rate in 2014, 2015, and 2016.
There are, of course, other factors at play. How many pills are prescribed and over what length of time are important variables. It is possible that Massachusetts’ doctors were prescribing more pills per prescription than doctors in other places. It’s also possible that Massachusetts had abnormally high prescription rates in the early 2000s, creating a population that was primed for a crisis. Unfortunately, we don’t have data that can speak to either of those variables.
Our best data suggests that while addressing prescriptions is central to fighting the opioid epidemic, a difference in the prescribing behavior of Massachusetts doctors does not appear to explain our especially high opioid-related death rate relative to other states. Over the next few years, Massachusetts’ opioid prescription rate is likely to remain relatively low as the state legislature recently passed opioid legislation encouraging more cautious prescribing. The bill, An Act relative to substance use, treatment, education and prevention, limits opioid prescriptions for both adults and minors.
Heroin also plays a key role, but not to a degree that is significantly different from other states.
Heroin usage is a critical factor in opioid-related deaths, particularly because heroin is often laced with fentanyl. 5 Heroin is the second most common underlying cause of opioid-related deaths in Massachusetts, behind only fentanyl (see Figure 5).
In tackling the opioid epidemic, minimizing heroin usage is a key strategy. But as with opioid prescriptions, heroin usage does not seem to account for Massachusetts’ outsized opioid-related death rate.
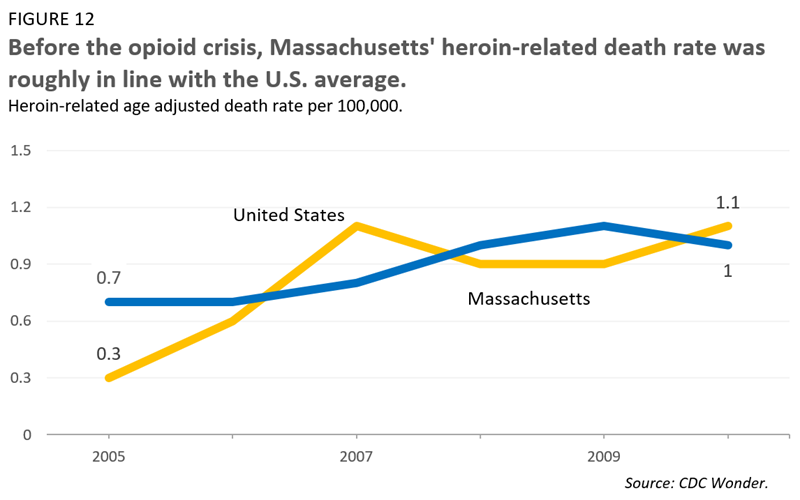
If Massachusetts had a higher share of heroin users than other states before the current opioid epidemic, there would be a disproportionately large number of people primed for deadly overdoses when fentanyl was introduced to the illicit market. The data, however, suggests that Massachusetts’ heroin usage was around the national average—and, in some years, below average.
Death rates are not, of course, conclusive evidence of great or little heroin usage. Unfortunately, data on heroin usage is incredibly difficult to collect and reliable data on drug use in general is increasingly rare. It is possible that Massachusetts had a disproportionately large heroin-using population but our healthcare system did a much better job of curtailing deaths than most other states.
That said, the most reliable public data we have suggests that Massachusetts’ population of heroin users was not abnormally large. In other words, heroin usage prior to the opioid crisis is likely not the reason why Massachusetts’ opioid-related death rate is so much higher than that of the nation.
1 - Data note: opioid-related deaths often have multiple underlying drug causes—one death, for example, might be caused by overdosing on heroin laced with fentanyl. This means that the number of underlying causes of opioid-related deaths exceeds the number of opioid-related deaths. For example, if we count 20,000 opioid-related deaths, 5,000 may be caused by heroin alone, 5,000 by prescriptions alone, and 10,000 by a combination of heroin and fentanyl. Therefore, there are 30,000 underlying causes (15,000 heroin causes, 5,000 prescription causes, and 10,000 fentanyl causes).
2 - See footnote above.
3 - Please note that this article uses the five places with the lowest opioid related death rates above zero.
4 - Also, please note that these unemployment figures are drawn from the ACS 5 year estimates for 2007-2011 (averaged on 2009) and 2012 to 2016 (averaged on 2014). We chose to use the ACS instead of CPS or CPS/LAUS data because CPS/LAUS has a more stringent definition of who is or is not part of the labor force, leading to what might be artificially low unemployment rates.
5 - Fentanyl, as previously mentioned, is much stronger than heroin and is often present in heroin without the knowledge of the user.